|
This is inspired by a talk delivered by Dr M R Rajagopal, Emeritus Chairman, Pallium India, as part of the seminar series “Palliative Care and the Motives of Medicine”, organized by the Harvard Medical School Department of Global Health and Social Medicine. This is written in his voice with his permission. The doctors attended to her leg and restored her sight. But were they solely responsible for giving her “life” back to her? What about the sweeper who provided food every day so that she did not have to consider suicide, as her son had suggested? What about the social media support that gave a roof over their heads? What is the motive of medicine? Are we here just to diagnose and treat diseases? Or is it a bit more than that? We may have come into it for different reasons but once we are in the field of medicine, we realize what a huge privilege it is to be part of healthcare. We find ourselves in a position to make the most difference to other people’s lives. We see people at the most vulnerable times in their lives and at times become the instruments to help them rise from the depths and smile again. To actually provide healthcare for all, we may sometimes have to travel over difficult terrain. At times, we have to strike a new path because at the other end there is somebody who belongs to 84% of the global population, without access to quality healthcare. They cannot get to us, we have to reach healthcare to them where they are, when they need it. Does that sound frightening?  A 55-year-old dying of cancer of the jaw. Image: Ruth Fremson, The New York Times. It takes more than a doctor Ironic as it might sound, I got to meet that helpless mother and son when I was leaving a World Palliative Care Day function. The 12-year-old boy had been sent with the hope that someone would be there at the function to help his mother. Her one leg was fully wrapped in an ugly bandage. And she was blind. She was about 40, a single mother abandoned by her husband. She had been a diabetic since the age of three. Diabetes had stolen her sight four years ago. A surgeon had said she would need an above-knee amputation. Of course, she was in significant pain, “like someone is cutting my leg with an axe.” She lived in a shack that belonged to someone else. She told me about a weekend when they had to starve. Hungry and frustrated, the son said, “Mom, let us kill ourselves. I cannot bear this hunger anymore.” Mom replied, “Son, today is Sunday. Let’s wait. I will find some way.” Somehow, they got across to a healthcare center. Luckily, they found a very humane doctor there who put them up for three months before I got to see them. They survived on the meal provided by a sweeper at the center every morning. They landed at the palliative care day function where I met them first because a kind nurse at the health center had directed them there. 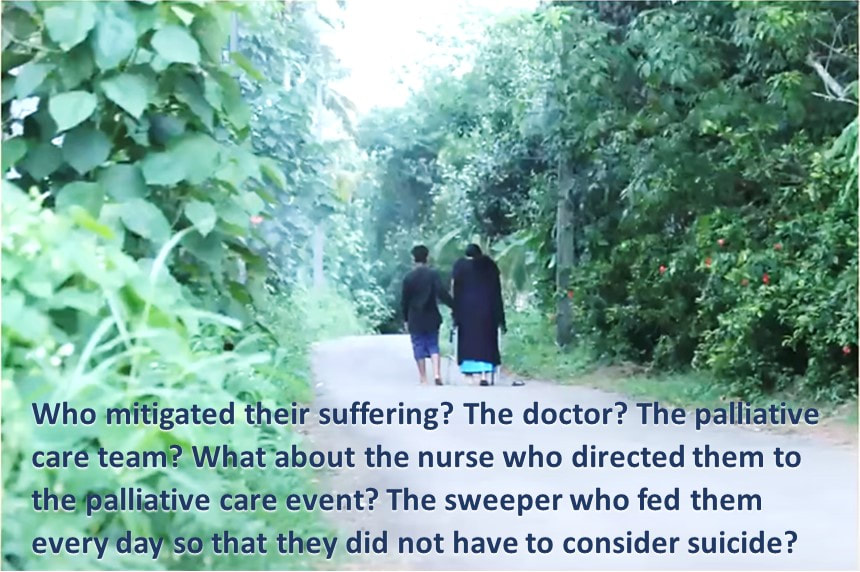 Image: Pallium India A definition distant from reality There are several definitions of palliative care today. Most of us working in the domain abide by what the World Health Organization had stated 21 years ago. Among other things, it prescribes palliative care for those with “life-threatening illness.” Let us go back to the mother we just met. She is diabetic; does she qualify? She is blind; does she qualify? More than anything else, does hunger qualify? The same persistent hunger that almost drove them to suicide? We cannot be rendered helpless by a definition. After all, such definitions tend to come from the 15% of the world that is rich and where all the meticulous studies happen. It gets applied to the 85% of people living in low-and-middle income countries in drastically different conditions. Do such definitions bind or liberate? Let us go back to the fundamental issue. What really is healthcare? When we keep someone’s heart beating, are we providing healthcare? What is the duty of the healthcare provider? The law does not define it in India. But the Indian Council of Medical Research, a statutory body, defines that duty as: “To mitigate suffering. To cure sometimes, to relieve often, and to comfort always.” And the ICMR emphasizes there is no exception to this rule. How many of us are aware of that definition? Do we practice it? Or do we stick to what we learn from the textbooks as dictated by medical institutions in 15% of the world, the high-income world? Palliation as mitigation If you are a healthcare professional and you have not been taught how to mitigate suffering or do not accept it as your primary responsibility, we in palliative care will be happy to help you. Not that we have all the answers. At least, we try. Because mitigating suffering is our primary motive. Opioids are one of the primary tools we use for relief from moderate to severe pain. In 2017, a Lancet Commission Report depicted access to opioids (which translates to access to pain relief) across the world. 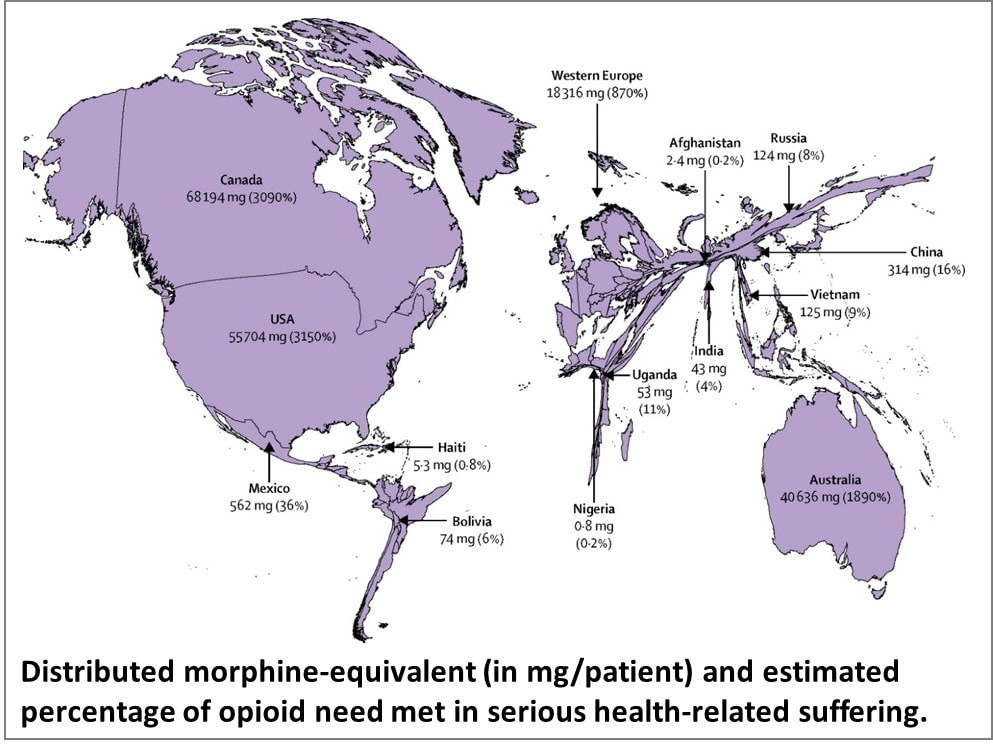 Source: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(17)32513-8/fulltext You can easily make out which country is obese, and which is malnourished when it comes to opioid access. The trick is to strike the right balance between easy availability and the necessary restrictions to prevent abuse and misuse. While we applaud western European countries for getting that balance right, let us not forget Kerala. In this tiny state right at the bottom of India, access to opioids is 16-times more than the national average. In the low-income Uganda, opioid access is three times better than what India claims. So, this shows it can be done. But why is it not happening universally? Is it because relieving pain or mitigating suffering is not a commercially attractive proposition for the industry that is at the heart of healthcare? Adding cost to suffering A study published by The Lancet on December 13, 2017, pointed at a vulgar disparity of life (to borrow Arundhati Roy’s expression). Not only are we not doing what we ought to be doing, but we are letting catastrophic healthcare expenditure add to the pain. The study aimed to estimate the global incidence of what they called catastrophic health spending. They measured this by the percentage of people whose out-of-pocket health expenditures were large relative to their household income or consumption. You are welcome to read the study for yourself. Personally, I was saddened and shocked to note that India was among the 12 countries burdened the most by the cost of health: more than 55 million Indians driven below the poverty line by what they had to spend on health; 38 million of them by cost of medicines alone. Such catastrophic health spending is not only for living with an illness; it is also for end of life—with the dying process excruciatingly stretched out over weeks or months in a desperate effort to prolong life at all costs. Are we afraid of death? Do we tend measure the “success” of medicine by how long it can keep death away? Is it difficult for us to accept that if life were a sentence, death is simply the full stop at the end of it? In January 2022, drawing on multidisciplinary perspectives from around the globe on the value of death, the Lancet Commission on the Value of Death argued that “death and life are bound together: without death there would be no life.” The Commission proposed a new vision for death and dying. It called for “greater community involvement alongside health and social care services, and increased bereavement support.” Cruelty of forcing to stay alive Moving away from professional studies and reports, let me narrate a personal experience. One of the professors who taught me medicine developed dementia. She was not swallowing well, so she was put on intravenous feed, against the advice of many of us. She would keep pulling the tube out. So, they tied her up. As every doctor knows, physical restraints can cause a 44-fold increase in the patient’s agitation. She did become more violent, and they promptly tied her up tighter. Eventually she was intubated and ventilated. The family had to walk in every morning and every evening for five minutes each, watching their beloved person being killed in order to be kept alive. Her daughter lamented, “Here was a person who gave a lot of love to a lot of people. Did she deserve to die this way?” Even as I write this, the daughter is receiving psychiatric treatment. I do not think she was affected so much by the loss of her mother as by the cruel way medicine kept her alive until the last excruciating moment. Why do our efficient, kind-hearted doctors refuse to accept that death is a part of life? Why do they hold on to the mistaken belief that it is their duty to prolong life at all costs? Is life merely a beating heart? The National Cancer Grid, a brilliant conglomerate of about 300 cancer institutions in the country launched the initiative Choosing Wisely India around 2020. The objective was to “identify low-value and/or potentially harmful practices in cancer care in India.” It intended to “facilitate a conversation between patients, clinicians, hospitals and policy makers on delivering high quality, affordable cancer care.” The aim was also “to reduce unnecessary interventions to improve overall quality of care, reduce patient toxicity and reduce the financial burden on both the patient and the system.” One of the recommendations was, “Do not treat patients with advanced metastatic cancer in ICU unless there is an acutely reversible event.” Laudable, isn’t it? But we all know what happens in hospitals. A friend, a senior neurologist, once remarked that our corporate hospitals are like fortresses that the poor cannot get into, and the rich cannot get out of. I do not think he was joking. A 2019 JAMA paper stated that in European intensive care units, 90% of all patients were taken off life support and offered palliative care once it was clear further treatment was futile. And, in comparison, what is the situation in India? Only 30% are taken off futile life support, that too any without palliative care support. As much as 70% of them die in ICUs. The end is stretched, hour by cruel hour for the patient, day by interminable day for the family. Helping us is up to all of us Let me get back to that woman and her son one more time. Yes, we treated her symptoms and pain. That was relatively easy but definitely not enough. One of us posted her story on social media and requested help. Help came. We now had money to pay for a caregiver while the patient underwent retinal surgery. After years, she got to see her son again. A diabetologist and podiatrist helped her get back on her feet, with support. She held her son’s hand and walked to a new home, where they are now supported by a monthly allowance, thanks to donations from the community. There is a huge gap between what healthcare is and what it ought to be. No doctor and no palliative care specialist can fill it by themselves. Does that mean we hide behind a definition and shut our eyes to the problem? The German physician Rudolf Virchow had said: “Medicine is a social science, and politics is nothing but medicine on a large scale. The physicians are the natural attorneys of the poor, and the social problems should largely be solved by them.” Our palliative care team is taking small steps. We are far from perfect, and it is a huge mountain to climb. But we are trying. By doing our best to support patients. By talking to the community about what we are doing and how they can help. There are many who want to help. But do not know how. Money is not the only way. I believe it is beginning to work. It has to. Right now, it is up to us to solve this social, or rather, humanitarian problem.  Image: Pallium India Every World Palliative Care Day is a special occasion when those who can help get together with those who need help to celebrate life. One such day, in the city of Thiruvananthapuram in Kerala, some 40 people came to the beach to wet their feet. So, what was special about that? These were all people confined to wheelchairs who could barely move out of their homes. It took four people to move each of them from home to the beach and back. So, it took about 160 people to make this happen. All doctors and nurses? No! They were students from two engineering colleges.
And what was their reward? One of the patients was a paraplegic who did not have normal sensation in her feet. She said, “the waves touching my feet is the best experience I have had in my whole life.” She couldn’t stop smiling. That was their reward. And that is the reward for all of us when the community joins hands with palliative care and medicine to mitigate suffering in the true, complete sense. We have a long way to go. We have just wet our feet.
0 Comments
 Your client meeting is at 10 a.m. in a city two hours away. There is a flight at 4 a.m. and the next is at 9 a.m. You can take the first and maybe finish some work on the way. Or you can request the client to reschedule. What would you choose? If you are the kind who would compulsively pick the 4 a.m. flight, skip sleep altogether (“might as well finish some pending reports and nap on the flight”), you are keenly aware of the rising number of people being laid off and the churn in the upper ranks of the corporate world. Or, more likely, you are yet another victim of workism. Not too long ago, journalist Derek Thompson described workism as “the belief that work is not only necessary to economic production, but also the centerpiece of one’s identity and life’s purpose; and the belief that any policy to promote human welfare must always encourage more work.” More recently, in his TED talk, Azim Shariff, a psychology professor at the University of British Columbia, noted that we tend to see a harder-working person as a “more moral”, better work partner, even though they add no extra value. He describes workism as a culture that forces all of us to participate and punishes us if we do not keep up. So, “we end up putting more and more in regardless of what comes out the other side.” The more laborious the job, the greater the appreciation even though there may be no direct correlation to tangible results. Everything else becomes less important. Workism at work A senior management consultant (“no names, please”), currently helping an MNC bring about a culture change observes that workism is a convenient term to describe what is happening at work. “Workism is a series of corporate behaviors that have seeped into organizations over a period of time. It requires a conscious change in senior leaders to break the mold—like focusing on smarter delivery than longer hours, like linking performance to results than efforts.” It even extends to everyday attire. “We have this senior leader from the old generation who refuses to be seen in anything other than his suit and tie whether he is addressing two people over coffee or a dozen in the board room. Then we have a whole bunch of smart youngsters always clad in denims and tees, who would rather walk in, deliver, and get out than hang around and be seen to be busy.” So, is it just a matter of bridging the generation gap? “There is a lot more,” my consultant friend tells me. “The biggest challenge before us is to define the goal. The goal is not about the hours we put in and what we wear at work. Surprising as it might sound, we found the youngsters to be clearer about the goal than the seniors; they have a surprising level of clarity on what they would like to do and not to, in their work environment and are willing to defy the stereotypes.” Inverting the pyramid The team is now attempting a radical management exercise where the newbies on the block would talk about the organization’s goals in informal meetings with the seniors. This inversion of the pyramid is sure to spark conflicts initially. “But It’s worth the try. What better way to motivate individuals than by declaring that we will measure you for what you deliver, not for all those hours you clock in. We expect this to usher in a positive entrepreneurial mindset and a sense of real purpose.”
Charlotte Kramer, author of The Purpose Myth: Change the World, Not Your Job notes that “70% of millennials want to quit their jobs on the grounds of lack of purpose, and this should be no surprise; the positions we take were created to fill our pockets (if we’re lucky), not to fulfil our dreams. To think otherwise is to suggest that one’s individual purpose can be matched with a corporation’s purpose.” The challenge for organizations today is to inject every member of the team with a common purpose regardless of one’s role. That’s where culture-change exercises are likely to become more common across domains—to change good old feel-right workism to measurable, no-nonsense purpose-ism. The organization should be sensitive to the individual’s purpose; the individuals should willingly buy into the larger team goal. You took the later flight but after persuading the client to meet you for lunch at place you knew was her favorite. Not once did you open the laptop, but by the time the desserts arrived, you had convinced her of the positives of working with you. In turn, she convinced you to stay back and address her top team where you did use the slides to make a convincing case. That quadrupled your workload, but you chose to sleep during the late-night flight back home. You knew tomorrow would be excitingly busy. Moral: There are times when the “lazier” 9 a.m. flights are more productive than the "harder working” 4 a.m. flights.  A coincidence is a matter of pure chance. Except when the timing of the incident defies logic and forces a non-agnostic glance up.
In the movie I am watching with my wife, a rich grandmother resorts to unconventional means (like spraying pepper on those trying to help) to rescue her servant’s daughter. The girl is smart, and they had formed a bond from the time the little one started shaping alphabets from dough. Then circumstances trap the girl in a situation where she is exploited. Of course, her conditions are different from that of Sush. Yet, that girl in the movie, teaching other children to speak English, did remind me of Sush, the real daughter of a real servant, who used to work at our place more than a decade ago. Sush, then seven, did not think much of my teaching, the stories I told her and even outwitted me in the “spot-the-place-in-the-map” game we used to play together. I was about to ask my wife, if the girl in the movie bore some resemblance to Sush, when the doorbell rang. I paused the movie while my wife went to open the door. It was Sush! She had come with a box of sweets and a sweeter announcement that she had passed her grade 12 exams with top marks. We invited her to join us in the room where we had been watching the movie. The cloud of economic uncertainty continued to hover over her family, now larger with her little sister. Yet, her sunshine nature was undimmed. She hoped to become a Master of Business Administration one day. She had picked up a small job where she was by now “comfortable”, giving her enough confidence to master business one day. Yes, she spoke fluent English and was very comfortable working on the computer at her job. Those are important skills, I lauded her. No, she was not very comfortable with numbers—neither math, nor accounts. Yes, she knows it may not be possible to do only what she likes; and she must do it well, whether she likes it or not. I applauded her spirit. The 18-year-old sitting and talking to us barely looked bigger than the little girl we knew then. Yet, her confidence was several notches higher. While we were talking, I located the blog I had written about her. She stopped talking when she saw the image of the little Sush on the monitor. Halfway through reading it, she started crying. The tears just wouldn’t stop. When she finished reading and got her tears under check, I asked her why she had cried. “I remember everything. I was always so happy coming to this room, being here. I must have this," she pointed to the blog. "Please give me.” I shared the link with her. And assured her she was welcome to visit us whenever she wanted. When I wrote “At 45-minute school with Sush” I had never imagined that I would be spending another 45 minutes with her 11 years later. For a change, this time she agreed to do some homework. She would write about her memories of those years. Perhaps she would explain those tears and share some of her dreams? She may or may not submit that homework. But when we resumed the movie, it was difficult to unsee Sush whenever that frightened, English-speaking, fragile-looking servant girl came on the screen. The movie ended happily, showing the girl being cared for by those who loved her. She was set to live happily ever after. We are sure so will Sush. And that would be no coincidence. Because Sush writes her own script. 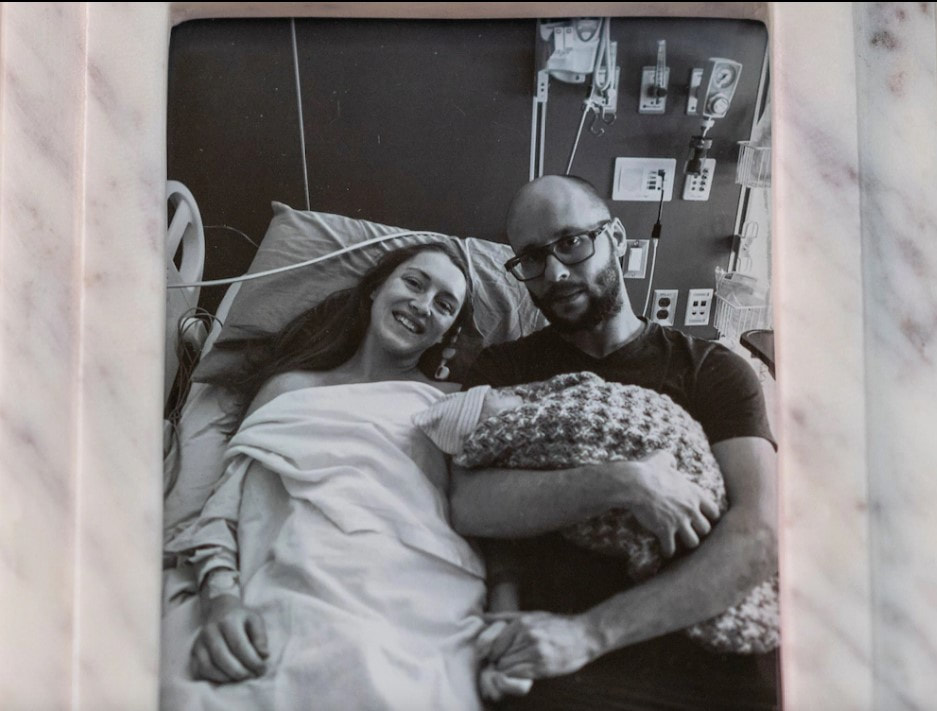 What does one do when the law that is blind to both medicine and compassion makes a mother carry a pregnancy though it is clear that the baby can only survive for a few hours? Baby Milo arrived in the world with no kidneys, underdeveloped lungs and a life expectancy of between 20 minutes and a couple of hours. He lived for 99 minutes. On March 3, 2023. Mother Deborah and her husband, Lee, had learned in late November that their baby had Potter syndrome, a rare and lethal condition. As long as their baby’s heart kept beating, the doctors would not honor their request to terminate the pregnancy. The new Florida law on abortion carries severe penalties, including prison time, for medical practitioners who run afoul of it. Everyone knew the baby would not survive. Yet, the parents had to wait for labor to be induced at 37 weeks. The Dorberts consulted with palliative care experts and decided against trying to prolong his life with high-tech interventions. The day before Milo was born, the Dorberts sat down with their son Kaiden to explain that the baby’s body had stopped working and that he would not come home. Instead, someday, they told Kaiden, they would all meet as angels. The 4-year-old burst into tears, telling them that he did not want to be an angel. After Deborah’s 12-hour labor, Milo turned out to be 4 pounds and 12 ounces of perfection, with tiny, flawlessly formed hands and feet and a head of brown hair. The obstetrician cut the umbilical cord that for 37 weeks had performed the functions Milo’s underdeveloped lungs and missing kidneys would now take over. Milo remained blue, swaddled in a blanket hand-knit by his great-grandmother. He never cried or tried to nurse or even opened his eyes, investing every ounce of energy in intermittent gasps for air. For 99 minutes that lasted a lifetime, they cuddled and comforted their newborn. At 11:13 p.m., a doctor declared Milo dead. At the service, the pastor from a local Lutheran church had a message for the congregation. “Not everything happens for a reason,” she said, echoing Deborah’s own rejection that the manner of Milo’s birth and death carried some special spiritual significance. Deborah wants other people to know what happened, how politicians intervened in decisions about medical care with a law that made doctors fearful of terminating even hopeless pregnancies. “If it helps another family or a mom, then good came of it because we’re all here to help one another,” Deborah said. “It’s not something easy to go through alone. You need all the support you can get.” I am not an expert in medicine or law. But I have a question for my compassionate friends in palliative care. How do you console, how do you care when law blocks your path, and medicine can only stand by? This is adapted from the report in The Washington Post. Please read the whole story here. Image from the report.
 Last Sunday, the day the world celebrated mothers, was no different for this mother. Her two sons, 33 and 31, are growing without hunger, pain, joy or sorrow, thanks to her. But do they even know her? Sometimes they do in the dining hall what they ought to do in the bathroom. Or do in the kitchen what they ought to do out in the yard. Radhamani would discover after cleaning up the mess that the younger was down after another epileptic fit. She would rush to find someone to mind the elder son and then rush to the hospital to fix the wound. She has just one persistent sorrow. That they don’t know her, her love. Every moment, she pines to hear them calling out to amma. There are times when she is cleaning the vessels or sweeping the yard, that she would hear that call. She would look up eagerly, only to realize nobody had called her. Writing erases pain Writing offers her relief. When she writes, her sorrows get erased. She has already published three books in Malayalam. She had a small government job. Father was a sweeper at a bank. Mother was a housewife. After finishing his work, in the afternoon, her father would go to pick jackfruit leaves which he would bundle up and take to the market to sell. Her most cherished moments were when she and her mother joined him to help pack up the leaves and carry those to the market. Radhamani had to displease her parents when she decided to marry her childhood friend, Raj. Both families objected. But the couple stuck to their decision. Radhamani and Raj had their first son nine years after marriage. They named him after the poet they both loved — Shelley. Two years later was born the second son — Sherry. The boys were a little late to start talking. When Shelley was three and half, their regular doctor felt something was wrong and recommended admission to a larger hospital. Both children were diagnosed to be autistic. The parents were advised to pray. “I realized the truth that they would need my help to go through life. Gradually I regained strength.” Radhamani had no option. By this time, her father was dead. Radhamani’s family returned to live with her mother. When both of them left for work, Radhamani’s mother would look after the boys. “The boys would be at a special school until the afternoon. Then mother would feed them and take care of them.” Waking up to cruel reality Radhamani’s world collapsed when her mother passed away. That’s when she came to know firsthand how tough it was to bring up the boys. When the boys were 8 and 6 respectively, a heart attack claimed Raj. That shock haunted Radhamani for a long time. Now, it has been 25 years since he moved on. She learnt that the boys had no clue about death when the family went through Raj’s cremation rituals. They were in no position to do whatever they were expected to do as sons. That whole night Radhamani spent crying. “I know when I die my sons will forget me within a week,” Radhamani states calmly. “Yet when I go out somewhere, they would be waiting at home. Waiting in the hope that I would get something to eat. That waiting is enough for me to live on. Else I would have taken my life long ago.” Finding refuge in words People tell her death lurks in her stories and poems. Radhamani knows. “It is my writing that keeps the thoughts of suicide away. That is why my writing smells of death.” “After I die, someone should adopt my children. I hope the government opens a facility to take care of such children in every district. That is my appeal, my prayer. Then I can die in peace.” This is based on a report dated May 14, 2023, in the Malayalam newspaper Mathrubhumi, written by Sajna Alungal. Illustration based on images accompanying the story.
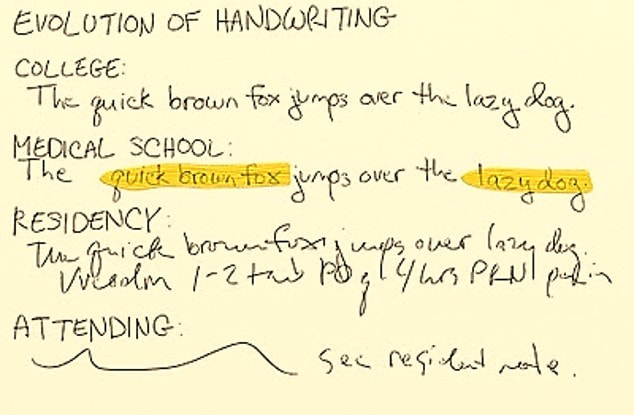 This was triggered by my recent visit, not to any doctor, but to the friendly, neighborhood laundry guy. He was scribbling a receipt for the clothes I had just given him when another customer, watching him write, remarked, “You should have been a doctor!” “Just need to get the degree,” the laundry man responded with a smile, “my handwriting has already qualified.” The joke continued when I crossed the road to get to the pharmacy. The pharmacist was deep in conversation with an elderly customer. They were both looking at a slip of paper that, going by the scrawl-style, might have been a written by the laundry man. I waited patiently as the conversation went over symptoms, likely diagnosis, the expected effect of the prescribed medicines and potential side effects. After sending the patient away (“when do you want me to come back?”), the pharmacist turned to me apologetically. “I don’t think he would have been able to read it even if he wanted to. Took me years after pharmacy college to read what doctors write. Of course, can’t expect every doctor to spend time explaining everything to every patient.” Grave consequencesThis joke is anything but new. But why has it persisted over decades? Why are doctors associated with bad handwriting? Not that it can be brushed off as a joke when “bad handwriting by doctors is responsible for 7,000 deaths every year” as cited by this old article. Worse, illegible handwriting is a major cause of “medication error,” that kills 30,000 people in the UK and 100,000 in the US, every year. Back in 2015, neurologist Dr Nomal Chandra Borah, founder of GNRC, observed that he was unable to decipher 25% of the prescriptions written by other doctors. He cited a case where a woman suffering from convulsions was admitted to his hospital. Another doctor “had prescribed her DUODIL—an analgesic, but what was bought and consumed was DAONIL—a medicine for diabetics. This was causing a sudden fall in her blood sugar levels, leading to the convulsions. Such a grave consequence, simply because of the illegible handwriting of the doctor….” Dr Borah applauded the guidelines from the Medical Council of India (MCI) asking doctors to write complete and detailed prescriptions “legibly and in capital letters.” However, he noted that it was hardly practiced and there was “no monitoring mechanism to ensure adherence.” (By the way, the MCI was dissolved on September 25, 2020, and replaced by the National Medical Commission.) What the doctors saidI decided to go to the source of the prescription and ask a few doctor-friends. Here are some bits from the responses. “Doctors are terribly busy. Would rather move to the next patient quickly than spend time to write neat and clean.” “People often doubt if I am really a doctor. Because anyone can read my prescriptions easily.” “It starts from the training days. You are supposed to go on rounds with the seniors and note the details of every patient. There is so much repetitive writing to do and very little time. You know the nurses would understand in any case. So, you just scribble to comply. And the habit sticks.” “When you are in college, there is a premium on neat handwriting. Your examiner is not your patient. Then workload and good old boredom take over. At least some seniors I know take the scribble as a strange status symbol. After all, it is to be read by another doctor who deals with another part of anatomy. Or a chemist. It is not meant to be read by the patient, they say.” “I knew a fellow doctor whose prescriptions could be deciphered only by a specific chemist. Not sure if he used some code.” “Technology is making a difference. Hospitals are getting paperless. Prescriptions are printed. Patient records are digital. You are complaining of bad handwriting still? Wait until AI gets here.” Some palliative medicine specialists I spoke to thought bad handwriting was a non-issue. “Every patient needs an understanding ear and a caring touch. Prescriptions come later.” Of course, I didn’t have the heart to tell them that the hero prescription now is AI and not EI (empathetic intelligence). Just Google itTalking of AI, surely bad handwriting ought to be something it can tackle easily? Apparently, it is! In December 2022, Google announced it was working on “an artificial intelligence (AI) and machine learning (ML) model that can identify and highlight medicines within difficult-to-read handwritten prescriptions.” Looks like we will soon have an app that can read any doctor and tell you what the doctor wants you to take to get better. Just what the doctor ordered! Or is it? Meanwhile, the doctor joke continues to bounce clean off the laundry guy. And the chemist offers human intelligence, experiential learning, and a patient ear to tell you what the prescription reveals. And no clinical touch needed; you can use your mobile wallet to pay for the medicine you hope will make you, well, well. Image: http://doccartoon.blogspot.com/2010/02/blog-post_07.html
 Is it possible to have one foot in surface science as an experimental physicist and the other playing bass in a heavy-metal band? Welcome to the life of Alessandro Sala! When he is not setting the stage on fire, Sala is “investigating the properties of nanostructured surfaces, 2D materials and organometallic molecules with a scanning tunnelling microscope.” When he is not exploring the intricacies of surfaces, he plays bass for Rhapsody Of Fire, a heavy-metal band “that has sold more than one million records throughout its 25-year history and regularly tours the world.” So, what’s the big deal in playing some music after work? His musical role “requires month-long absences from the lab, early-morning flights and dark leather clothes.” (Wonder if the molecules would act differently if the scientist observing them wore dark leather clothes and carried a bass guitar!) Science and music Writing in Nature, Sala says, “Good time management is key to having the best of both worlds.” If that sounds like a cliché, it is an art he has scientifically perfected over the years. His strategy is to find separate spaces for music and science. “I accept master’s candidates and temporary lecturing positions only if no big tour is scheduled in the following semester. I train my postgraduate students to be completely independent, so they can keep working when I travel.” And he attends conferences only in May, June, September and October; the band tends to tour in the other months. He arranges his parts in new songs mentally over a couple of months and condenses all recording sessions into a couple of weekends. He shares his musical commitments with his co-workers and carefully plans lab activities so that work and music are always in tune. Yes, Sala does attend lab meetings remotely so that he is always updated. No rehearsals while doing lab work, except that “while I’m immersed in an experiment; I do listen to good music, though.” Delightful duet Has one profession had an influence on the other? His colleagues are happy to use his scanning tunnelling microscope during his scheduled absence. Also, “in the lab, everybody is capable of using every instrument, and often we help each other on our scientific projects.” In the music industry, all events from composing new music to live tours are routinely planned around two years ahead. “I treat research branches like albums: every couple of years I revise them critically, and I am not frightened to start a new one, if needed.” “When I come back to my lab after a month of sleeping on a tour bus, my mind is ready for new scientific ideas, and I feel free to dedicate myself to a scientific task within a well-defined time frame.” How does one describe Sala’s life—a symbiotic symphony or a delightful duet? Source: https://www.nature.com/articles/d41586-023-00991-5
Composite image: 1. Alessandro Sala's image by Esther W. Pink from Nature; 2. still of animated image of scanning tunnelling microscope from ArchimedesBerlin.  There is the real game of life for most people, and there is the virtual life of massively multiplayer online gaming that is the only real thing for many. A recent report suggests that gaming will soon be the real thing in life, and everyone would be a gamer. Brent Baldwin, once a gamer himself, fervently hopes this future will not come to pass. In Baldwin's story, “a collection of so many things from my own life”, the gamers in the future are a lost generation, educated but unemployed, living “in a world too expensive and too hot for in-person gatherings.” Yarro, the central character, lives in a bare minimum pod with no kitchen. For Yarro, “the lack of a kitchen meant more room for a fully immersive gaming rig, which was the height of human existence.” He hates to go the place where his dad lives (“Miss you, son”) because he does not want to “endure the sun and the heat outside his pod”. Also, because Yarro doesn’t want to run into anyone “who would pester him about ‘not calling’ or ‘how have you been’ or ‘I’m so sorry about your mom’.” Yet he ends up going there because Sisho, a member of his “posse” had uncharacteristically not logged in for two days. Imagine! A gamer not online! He got to know from a fellow gamer that Sisho was in a hospital near his father’s place. Sisho had almost died from “nutritive failure.” In non-gaming, real-life words, Sisho was so engrossed in the game that he did not pause to eat and had almost starved to death. After leaving the hospital, Yarro goes on to visit his father. Standing in his childhood home, Yarro remembers his parents’ laughter. “How it used to seem so fake, until it was absent. For most of his life, all Yarro had really wanted was to get into a gaming rig and explore other worlds, but for a moment he imagined himself as his Dad, alone day after day. Sisho had the posse waiting for him. With Mom gone, Dad had no one.” Do read Yarro's story and ponder about the future that awaits all of us. A few minutes ago, I came across a scientist’s prediction that technology will make humans immortal by 2030. By 2045, “we will multiply our effective intelligence a billion-fold by merging with the intelligence we have created.” Can we harness some of that artificial intelligence to undo the damage we continue to wreak on the outside? And to restore the fragile love and fraying care within us?
 That is one animal which does not feature in this documentary. Yet, its call to heed the elephant in the room is not a whisper but a shriek.
Thanks to the push provided by the Oscar-fuelled social media, I finally saw The Elephant Whisperers a couple of weeks ago. Loved it! Made me relive the only time I had the opportunity to give an elephant a bath, in Dubare Elephant Camp, Coorg. I have always been in love with the gentle giants. Oscar or no Oscar, I would definitely watch the documentary again for Raghu and Ammu, and the beautiful visuals. There are no such beautiful visuals in the documentary I saw a couple of days ago--All That Breathes. No, this is not an attempt to compare the two documentaries. They deal with the same truth we live, but in different ways. While The Elephant left me feeling good, Breathes left me feeling guilty, uneasy. I don’t think I will ever be able to look a bird in the eye after watching Breathes. Let me not spoil your experience of watching it and forming your own impressions. Just think of all that breathes with us on this planet. And somehow surviving in the filth that has become our ecosystem. We struggle to survive even with fellow members of our species. While we orate, shout, fight and burn, who has the time to worry about birds dropping from the sky? How can we possibly keep breathing when we consciously and unconsciously create conditions that make it difficult to our fellow residents to live in health and peace? Kites are using cigarette butts as insect repellents in their nests. Should we applaud their ingenuity or be ashamed by our own self-centred callousness? All That Breathes is set in Ghazipur, where I was some years ago. Then as now, working away in the shadow of the infamous garbage mountain, artisans create pieces of art from waste. Perhaps, there is hope yet? Or should we tell that to the birds?  “The earthquake was in Afghanistan,” the old fruit seller said, “but Delhi too was shaken.” He was handing over the second plastic bag my friend had demanded as a backup for the first one bulging with apples and mangoes.
My friend smirked and walked with me to the car. “What did he mean by that?” I asked. “Oh, he is nice but a little mad,” my friend replied. “He does not like it when people ask for plastic bags to carry the stuff they buy from him. He used to plead with everyone to get their own cloth bags. He gave up when people stopped buying from him. Crazy guy!” What does that have got to do with the earthquake? “He keeps lecturing that we are all one. Earth is gifted to us to by God, it seems. We must all protect it or we will be left with no home. As if, if I stop using a few plastic bags, the planet would be saved. Ha!” “I doubt if he is even literate,” my friend continued, “but he talks of climate change. Yes, the very words. Climate is changing because God wants to give us a warning, it seems. This earthquake must have been God shaking his fist … ha, ha, ha!” He was still laughing when I dropped him off before his gate. I think I will carry a bag or two with me from tomorrow. And I will walk all the way. Why bother with a car when I am supposed to be on my morning walk. No, I am not thinking of that crazy old man. But why am I thinking of my baby born last month? |
AuthorVijayakumar Kotteri Categories
All
Archives
April 2024
|
 RSS Feed
RSS Feed